| Grading Stenoses |
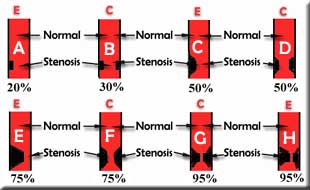
The diagram below show 8 tubes that represent coronary arteries with either eccentric (E) or concentric (C) stenosis of varying severity. For example A has an eccentric stenosis. The black area within the red tube is equivalent to a stenosis that compromises 20% of the lumen of the artery. In other words, the lesion diameter is 20% of the normal vessel diameter. On the other extreme, tube G shows that the stenosis is concentric and occupies nearly 95% of the lumen (as compared to the adjacent normal artery. The other tubes represent other degrees of stenosis. |
 |
Many experienced cardiologists are able to visually determine the severity of stenosis and semi-quantitatively measure the vessel diameter. However, for greatest accuracy, digital cath labs have the capability of making these measurements and calculations with computer processing of a still image. The computer can provide a measurement of the vessel diameter, the minimal luminal diameter at the lesion site and the severity of the stenosis as a percentage of the normal vessel. It uses the catheter as a reference for size. Note that cardiac catheters come in various outer diameters that are referred to as "French" units. One French = 0.33 or 1/3rd mm. Thus, a 6F (French) catheter has an outer diameter (OD) of 1/3 x 6 = 2 mm, while a 9F catheter has an OD of 1/3 x 9 = 3 mm. A table of various French sizes are shown below:
|
|
FOR AUDIO: Click the Speaker Icon to "unmute" Audio The animation on the left shows varying severity of concentric stenoses involving a model of coronary arteries. It is apparent that since the narrowing is concentric, the stenosis does not change appreciably as each artery spins around it's respective axis. Thus, the lesion or stenosis maintains a relatively constant proportion to the normal artery as it is viewed in various RAO, LAO, cranial and caudal projections. |

|
FOR AUDIO: Click the Speaker Icon to "unmute" Audio The animation on the left shows varying severity of eccentric stenoses involving coronary arteries. It is apparent that since the narrowing is eccentric, the stenosis does change appreciably as each artery spins around it's respective axis. Thus, the lesion will appear to vary as it is viewed in various RAO, LAO, cranial and caudal projections. The pictures in the top row show the cross-section of each artery as seen at the level of the lesion. While the lower row represents the same vessel in the longitudinal plane. Remember that this view is analogous to the coronary angiograms. |
| Many times, it is difficult to grade a
stenosis as having a single percentage value, i.e., 50%, 70% etc.
In such cases, one has to resort to a range such as 30-50%, 50-75%,
75-95%, etc. Minor lesions of a 10-20% severity is referred to as
10-20% luminal irregularities. Arteries that are totally occluded
are referred to as total or 100% occlusions.
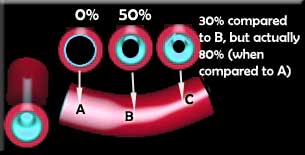
The above schema is simplistic and may not be applicable when a vessel is diffusely diseased, as shown in the example below. Level A represents a normal reference segment of the artery. At level B, there is a concentric 50% stenosis. It then tapers even further at level C. The severity of the stenosis would be 30% if one compared it to the adjoining segment B but is actually 80% when compared to the normal segment A. |
 |
| This phenomenon was first brought to our attention by
post-mortem examination of cadaver coronary arteries and can be confirmed
in the cardiac cath lab by intra-coronary ultrasound (ICUs). A decision
to proceed with a percutaneous coronary intervention in such cases should
be dictated by the clinical picture, objective data (stress test imaging,
if available), ICUS evaluation or hemodynamic assessment with a pressure-wire,
if available. The minimal luminal diameter of the vessel at the site
of the lesion may also be invaluable. Length of the lesion:
Lesions or stenosis may be discrete, short, or long. One can make
a rough assessment of the length of the stenosis by comparing it to
the diameter of the catheter. For example, if it is 3 times the diameter
of a 6F (2 mm) catheter, then the lesion is roughly 3 x 2 = 6 mm.
However, when one recognizes that the stenosis and catheter are in
different planes, it is obvious that this method is not reliable.
Accurate measurement of a lesion length during a percutaneous intervention,
such as coronary stenting, can be made by comparing its length to
that of an angioplasty balloon or a guide wire with radio-opaque markers. |
| Grading Stenoses |